Last Updated on February 17, 2023 by Andre Panagos M.D.
The Pitfalls of Diagnosis by MRI.
MRI (magnetic resonance imaging) is a non-invasive radiology imaging tool. It is a medical test that uses radio waves instead of ionizing radiation, such as x-rays and CT scans. These radiowaves produce detailed images of the human body. This imaging study is particularly helpful in looking at complex areas, such as the lower back, called the lumbar spine. It is considered the “gold standard” for diagnosing spinal problems such as low back pain, neurogenic claudication, sciatica, and herniated discs, but it is not perfect. MRI is the best test imaging tool for looking inside the bones, intervertebral discs, foramen (holes that the nerves emerge from), facet (zygapophyseal) joints, spinal cord, nerve roots, and the soft tissues such as the muscles, tendons, and ligaments. Yet, sometimes, the MRI results are unremarkable when the patient is still in pain.
Spine degenerative changes associated with age
Spine “abnormalities” may not be the cause of back pain but are rather normal degenerative changes related to aging. A classic study found that more than 50% of a group of 98 people without symptoms of back pain, ranging in age from 20 to 80 years old, had spinal abnormalities. For instance, a prevalent spinal abnormality such as a disc herniation at the L4-L5 disc level on a lumbar spine MRI may not be the cause of pain. Another study notes that severe disc degeneration at 18 years of age has a higher risk of overall chronic back pain by the mid-30s.
The majority of back pain is not serious
Up to a quarter of all visits to primary care doctor visits are for low back pain. You may feel your lumbar spine is in grave danger if you experience severe low back pain. You might ask your doctor to take an MRI to alleviate your worries. Most lower back pain is not caused by serious conditions.
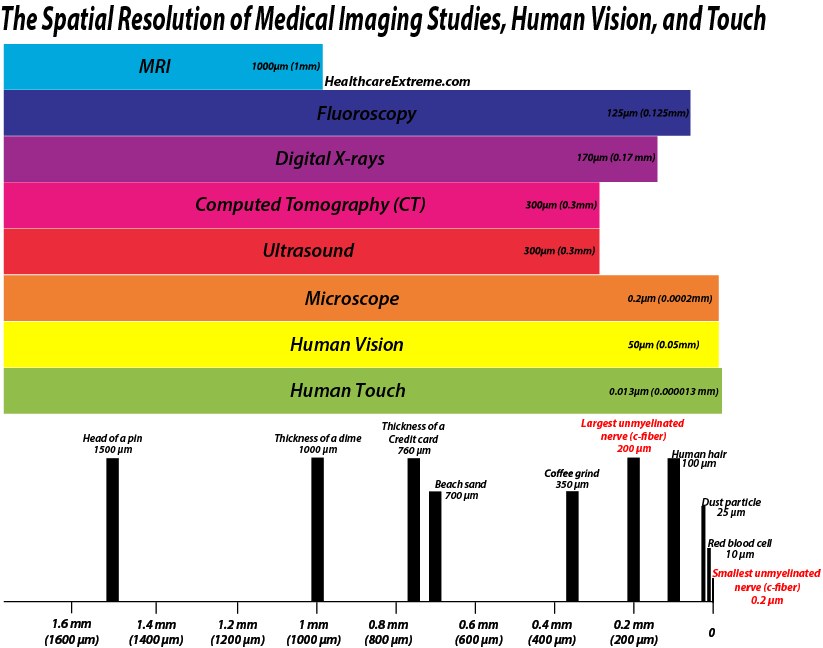
What is the resolution of an MRI study, and why can’t it pinpoint my pain?
A classic study found that less than 50% of a group of 98 people without symptoms of back pain, from 20 to 80 years old, had a normal MRI. Using only MRI to diagnose pain yielded poor results in a study of patients with lumbar spinal stenosis who were presumed to have pain associated with the narrowing of the central spinal canal.
Magnetic resonance imaging studies have a resolution down to 1mm, which is the thickness of a credit card. This is an amazing resolution, but more minor injuries can be overlooked. These injuries include annular tears of the discs, nerve root traction, joint or spinal ligament instability, muscle tears, ligament tears, or tendon tears, known as tendinosis.
The nerves that transmit most pain signals (nociceptors) from the skin surface down to the central nervous system (CNS) are called C fibers. They have a diameter ranging from 0.2 micrometers to 3 micrometers. There are four types of C fiber nerves that respond to different high-intensity mechanical, chemical (inflammation), and thermal stimulation. If any of these nerves become active, they can create a regional sensitization signal which some people call referred pain which makes it very difficult to identify the original pain generator, especially when it is severe.
Common causes of back pain not seen on MRI
Microscopic injuries
The sensitivity of MRI for assessing abnormal tissue is considered excellent, although some physicians question if this is the case. Although no research compares MRI sensitivity in lumbar spine injuries, we can extrapolate findings from whiplash research for clarity.
In a classic study by Taylor in 1993 involving the cervical facet joints, physicians compared x-rays to very detailed histological evaluations of the joints to assess for tissue damage. They found that x-ray studies did not pick up the microscopic injury.
Another study by Uhrenholt in 2002 reviewed the literature on fatal lesions after road traffic accidents in the cervical spine with x-ray, MRI, and CT scan and found evidence to suggest that subtle lesions in the cervical intervertebral disc and facet (zygapophysial) joints may be underreported.
Referral pain
Pain from structures near the lower back, such as the hip or sacroiliac joint, or far away, such as the cervical spine, may mimic low back pain. Lesions in the hip may cause hip pain and increase pressure along the lower back, greatly worsening an otherwise mild discomfort.
Protective adjacent tissues
Structures that are damaged or degenerated can be protected by adjacent healthy tissues or osteophytes (bridging pieces of bone that limit motion). Yet, if the muscle tension is excessive, it could exacerbate the pain associated with minor injuries leading to severe pain. Alternatively, pain-related muscle inhibition or weakness can weaken the muscle, resulting in less protection from excessive joint forces leading to more significant pain.
Biomechanics
Biomechanics can also be altered, resulting in greater forces across the lower back. For instance, any abnormalities in the pelvis and/or foot result in improper lower back joint and muscle positioning, resulting in tissue overload and eventual pain.
Psychosocial
Psychological factors may also play a role in pain behavior reflected in interactions with work colleagues, medical practitioners, insurance companies, and disability programs. Increased worry results in increased muscle tension which places greater tension on the spinal tissues.
What does an MRI scan show well
Magnetic resonance imaging is an excellent tool to assess specifically:
- Spinal alignment
- Nerve inflammation or swelling
- Spinal fractures (vertebral body fractures)
- Congenital or developmental abnormalities
- Spinal cord injuries
- Infections or abscesses
- Benign or malignant spinal tumors or masses
- Abnormal blood vessels
- Severe narrowing in the central (spinal stenosis) or foraminal canals (foraminal narrowing)
- Large disc herniations
- Facet (zygapophyseal) joint arthritis
- Progress following spine surgery.
When to order an MRI
The details on an MRI scan must correlate with the patient’s situation to be valid.
- The patient’s symptoms (such as the severity, duration, and location of pain)
- Abnormalities in the physical examination
Up to 60% of patients with symptoms longer than 6 weeks who seek healthcare report significant improvement or resolution.
Disc herniations can even decrease in size (resorption) in over eight weeks. Therefore, a spinal imaging test may not be necessary.
Great doctors combine their entire history and physical examination findings to diagnose and create an appropriate treatment plan. This is associated with the best treatment options with the best chance of pain relief, including physical therapy, pain management, or orthopedic surgery providers.
The timing of the MRI scan is also important. An MRI scan is urgent if a patient is experiencing any of the following, which are termed “red flags”:
- Severe pain
- Sudden or progressive bowel or bladder incontinence
- Progressive and unexplained leg weakness and loss of the ability to walk or stand
- Progressive, unexplained and severe spinal pain such as occurs with spinal fractures from osteoporosis, the use of steroids, or cancer
- Trauma or injury
Indications that you should have an MRI.
- If the pain persists for more than six weeks, is worsening, or you are considering a spinal injection or other intervention.
- If the low back pain worsens or persists for more than 3 to 6 months and has not responded to conservative treatments such as activity modifications, oral medications, and physical therapy.
- Back pain that is accompanied by weight loss, nausea, vomiting, fever, and chills which may be related to an infection, tumor, or mass. An MRI with and without contrast differentiates areas of increased blood flow (infection or tumor).
- Pain that has not changed or is worsening after back surgery. In this case, an MRI is ordered with and without contrast to assess for a hematoma, cerebrospinal fluid leak, seroma, infection, or scar tissue.
Patients can also experience spinal pain that is not consistent with MRI findings. Further testing may include diagnostic nerve or joint steroid injections, electromyography (EMG)/nerve conduction studies, and x-ray studies.
Sometimes, but not always, subacute pain (lasting between 4-12 weeks) and chronic back pain (lasting 3 months or more) are rare signs of an urgent lumbar spinal condition. Less that 1% of patients suffering from lower back pain and who are diagnosed and treated by their primary care physician require spine surgery.
What to expect from your MRI study
How to prepare for your MRI
You can usually eat and drink before the test and take your usual medication unless otherwise directed. Leave your jewelry, including body piercings, watches, and/or dentures, at home or prepare to remove them before the study. You will also need to remove hearing aids and glucose pumps. It is essential to take note of any metallic implants such as cardiac or other blood vessel stents or joint replacements. Some implanted electronic devices may preclude you from having the MRI or may need to be temporarily turned off before the MRI. Also, if you have a contrast allergy, please inform the physician or MRI technologist. Mention if you have claustrophobia. Sometimes people find out they are claustrophobic for the first time in an MRI machine.
What to expect in the MRI machine
Lumbar MRIs take from 30 minutes to 2 hours to complete. Your entire body may be in the MRI machine, but only the part of the body surrounded by the imaging coil will be imaged. To image another area will require a separate MRI session. If you need medication to relax during the MRI, such as valium or other sedatives, you may need to be accompanied home after the test.
You will put on a gown and lie on a table. Then slowly slide into a giant bagel or donut-shaped machine. Most of your body will be in the central tunnel of the MRI machine if imaging the brain or spine. You may only need to insert your limbs into the MRI machine for extremities. The MRI technician will guide you through the test.
You may require contrast dye which will be given to you through an intravenous catheter inserted into your hand or arm.
The strong magnetic field aligns the magnetic fields of the protons in the water in your body. When the magnetic field is turned off, the protons return to their usual alignment and release energy detected by the MRI.
Expect a loud banging noise during the test, which will be muted somewhat with headphones or earplugs. You will also be expected to lie very still during the test.
After the test, a radiologist will interpret the results and summarize them in a report sent to the ordering physician. The results of the test can be available as fast as the same day, but it usually takes several days to be completed.
Risks of an MRI
MRIs are considered very safe but precautions are taken to reduce the risk of severe injury.
The strong magnetic field can attract at high-speed metallic items, which may become a projectile resulting in injury.
Metallic thread within high-tech clothing may heat up, resulting in a burn.
Implantable electronic devices such as pacemakers, defibrillators, and spinal cord stimulators and/or the leads may move out of place or again cause burns.
Hearing loss or tinnitus can also occur from the loud banging noise.
Pitfalls of MRI
MRIs are not appropriate for all patients as it uses powerful magnet technology, which may not be safe for some patients. MRI is not recommended for pregnant women or those with metal in their bodies, including non-MRI compatible spinal cord stimulators, pacemakers, other implantable stimulators, or leads.
Contrary to popular belief, very low quality evidence exists for the diagnostic accuracy of MRI in specifically identifying the symptomatic lumbar disc herniation. In another study, other than Pfirrmann disc degeneration grade or vertebral body spurring, no MRI characteristics were reliably identified that correlate with acuity of symptoms.
Depending on who is reading the images, MRI results can be unpredictable, so good physicians and surgeons examine the actual MRI results with their patients and do not just read the reports.
Choosing your MRI facility is critical
Many factors determine if an MRI is completed and interpreted correctly. Pitfalls that impact the magnetic resonance imaging (MRI) results include:
- Cooperation of the patient
- Facility accreditation by the ACR (American College of Radiology)
- MRI magnet strength (1.5 Tesla vs. 3 Tesla machines)
- Age of the MRI machine- as older machines may miss more pathology
- Quality of imaging coil placed around the specific body part to generate the image
- Quality of imaging program used to control the MRI
- The skill of MRI technician
- Programming for scanning the specific body part and clinical condition
- The skill of radiologist who reads your scans
There has been a shift away from history and physical examination towards relying on MRIs to diagnose patients to the detriment of patient outcomes.
Impact of MRI Magnet Strength on Image Resolution

A negative scan does not mean there is nothing wrong; if you have progressive alarming symptoms, consider a second opinion.
Cost of MRI
MRI testing can be expensive. . The Kaiser Family Foundation data found that an MRI in the United States cost $861 in 2018. The United States is the most expensive country for an MRI study. The cost in the Netherlands was US$190 in 2017, making it the cheapest country for MRI studies.

